

KEYWORDS
lifestyle behaviour, long-term survival, Mediterranean diet, physical activity, smoking
INTRODUCTION
Our knowledge about the role of lifestyle behaviour on health and disease derives from population studies started in the middle of the last century. Most old studies dealt with the search of biochemical or biophysical measurements (e.g., serum cholesterol, blood pressure [BP]) as possible predictors or causes of diseases, but soon behavioural characteristics were also taken into account. Among these, a pivotal role was played by smoking habits, physical activity and dietary habits.
The main contributions are linked to coronary heart disease (and cardiovascular diseases in general), and to cancer, but findings dealing with all-cause mortality are becoming more and more common.
The literature is now rich with many contributions that consider either the above behaviours one by one or else combined.
SMOKING HABITS
The role of cigarette smoking on health and disease has been explored for decades, and was among the first behavioural types to be studied. The universal conclusions led to its strong, probably causal, association with the occurrence of lung cancer, and probably other cancer sites, coronary heart disease and other cardiovascular conditions, chronic bronchitis and allied conditions. The mechanism is complex and somewhat different depending on the disease. The documentation is huge: it is enough to quote the 50-year follow-up study on British doctors conducted by Doll and Peto [1] and one of the many systematic reviews on the bulk of the acquired knowledge [2].
Cigarette smoking is not a physiological habit and in contrast it has taken an enormous amount of effort to reach some partial results in some countries, but not everywhere. In some countries, smoking habits are still reported to be on the increase.
PHYSICAL ACTIVITY
Physical activity has also been studied for decades as a possible behavioural characteristic, mainly for the promotion of cardiovascular health. Many of the early studies were related to working physical activity, but later the approach was radically changed by studying leisure time physical activity, due to the drastic reduction of motion habits related to work occurring mainly in western societies. Present knowledge has led to the conclusion that a certain amount of physical activity is protective against coronary heart disease, perhaps other cardiovascular conditions and other diseases [3,4]. There has been much discussion in order to identify the minimum levels of activity that are useful for protection and are also safe. The present orientation is that moderate daily physical activity such as walking or biking 30-45 min a day has the same protective effects as performing more intense sports activities two or three times a week [5]. It is not completely clear whether physical activity is beneficial for diseases other than cardiovascular ones, but at least for diabetes it seems so. Benefits have also been documented from the psychological point of view.
Physical activity produces its beneficial effects through mechanisms that involve the physiology of the cardiocirculatory system and glucose and lipid metabolism in general, and the coagulation process.
DIETARY HABITS
After the simple observations of the early 1900s based on the so-called geographical pathology approach, the first systematic study of dietary habits and disease (focused on coronary heart disease) was made by the Seven Countries Study of Cardiovascular Diseases which began in 1957 and is still running. The initial hypothesis was linked to the relationship of saturated fatty acids on serum cholesterol and of serum cholesterol on the occurrence of coronary events. Initial findings based on ecological analyses showed the strong relationship of saturated fat intake with coronary heart disease incidence and mortality across different populations of different cultures [6]. Later, the approach turned to the dietary pattern analysis of food groups [7], that prompted the identification of the so-called Mediterranean Diet, roughly characterized by a predominance of plant versus animal food intake. Such a diet seems beneficial against several morbid conditions, including coronary heart disease, cancer and others. Certainly, many mechanisms intervene in the process, linked at least to the influence on lipid metabolism, the coagulation process and the antioxidant properties of the Mediterranean Diet.
Subsequently, many other studies, carried out in Mediterranean and non-Mediterranean countries, confirmed that within any population it is possible to identify subgroups of people who follow dietary habits similar to those described as the Mediterranean Diet, and are protected against major morbid conditions and all-cause mortality. One of the early studies of this type was carried out in Greece [8]. Presently, many other studies tend to refine these concepts and to find a better definition of the ideal diet for health purposes.
An additional important point, that is not always focused on the description of the Mediterranean Diet, is the need to reduce the daily consumption of salt [9]. Presently, in most populations, its use exceeds (by two times) the physiological needs, favouring the elevation of blood pressure and perhaps the evolution of atherosclerosis. There is indeed increasing evidence for additional blood pressure-independent pathways linking excess salt intake to the process of atherosclerosis, and some meta-analyses of randomized controlled trials have shown that a moderate reduction of salt intake is associated with a reduction of blood pressure and, consequently, with a reduction of cardiovascular and cerebrovascular events in hypertensive individuals [9]. According to recent European Society of Hypertension/European Society of Cardiology (ESH/ESC) guidelines for the management of hypertension, all patients should be instructed to reduce dietary salt intake to the level of 5 g/day, whether they are under current antihypertensive drug regimens or not. However, the response of patients to these recommendations is heterogeneous, mainly due to variable compliance with the doctor's prescription, and, to a lesser extent, to different individual BP salt sensitivity [9]. There is accordingly, plenty of room to intervene favourably with a potentially high impact for prevention.
Another important point, frequently ignored, is the adverse effect of trans fatty acids that are artificially produced and introduced in prepared foods, although this is a declining trend, at least in some countries [10]. Labels of food composition must be the guidance for avoiding its use.
COMBINED BEHAVIOURS
Studies based on combined behaviours can be found in the literature. A selection of ten contributions from the USA, Canada, Australia, China, Korea, Singapore and a dozen European countries and one meta-analysis are examples [11-22]. The three basic behavioural risk factors, i.e., cigarette smoking, physical activity and diet, although measured and defined, time after time, using different techniques and criteria, have been considered in all studies. Some investigations also included alcohol consumption (independently from diet) and some indices of obesity, such as body mass index and waist circumference or even other behaviours. The duration of follow-up was variable but usually covered 10 years and up to 24 years, except one study that reported follow-up data of 50 years. All-cause mortality was the endpoint analysed most, but some contributions also considered cardiovascular diseases, coronary heart disease and cancer mortality, while only one presented data on the incidence of major coronary heart disease (CHD) events. The reported relative risk of people with healthy behaviours versus those with unhealthy behaviours provided a wide range, from 0.23 up to 0.76. However, this depended upon the number of combined behaviours (up to six), the kind of endpoint, age range, gender, and duration of follow-up.
The conclusion from the above reports is that, despite differences in risk factor measurement techniques, age range, gender, geographical and cultural settings, duration of follow-up and endpoint definition, the outcome seems relatively homogeneous across the various experiences. A recent meta-analysis confirms and reinforces this impression [21].
OTHER PROBLEMS LINKED TO PREVENTION ACTIVITIES
Clearly, the role of physiological behaviours may not be enough to produce beneficial effects, since measurable risk factors, such as blood lipids and high BP, might only partly be influenced by lifestyle behaviour. Therefore, attention should be paid, if needed, to control these risk factors by the use of drug intervention, which becomes an integral part of preventive action. Detailed indications and guidelines are available from expert committees of various scientific organizations: these have also been quite recently reviewed and commented upon [23]. In particular, it appears that in Europeanpopulations the ESC/EAS guidelines from 2011 [23] (recently updated for application to clinical practice in 2012 [24]) seem to be the most wide-ranging, pragmatic and suitable choice for appropriate preventive measures.
A DIDASCALIC EXAMPLE FROM PERSONAL EXPERIENCE
A comprehensive dedicated example is reported below from the personal experience of the authors. We also present these data so that they might be used pragmatically by practising cardiologists to foster lifestyle changes aimed at prolonging life expectancy in middle-aged individuals. This example deals with the Italian Rural Areas of the Seven Countries of Cardiovascular Diseases study, comprising 1,712 middle-aged men studied during a follow-up of 50 years when the cohort was almost extinct, with a final survival of 2.5% [25]. For the purposes of this analysis, three basic behavioural characteristics were considered, i.e., smoking habits, physical activity and dietary habits, as related to mortality and survival over 50 years.
Cigarette smoking habits were derived from a standard questionnaire. Three classes of smoking habits were used for analysis: non-smokers (including ex-smokers), moderate smokers (less than 20 cigarettes per day), heavy smokers (more than 20 cigarettes per day). Physical activity was derived from a questionnaire that matched some simple questions with the profession, classifying people as sedentary, moderate or vigorous. The mean caloric expenditure of each class has been estimated by two different methods [19]. Such classification was confined to work activity, since in the middle of the last century leisure physical activity was practically nil in the explored rural environment.
Dietary habits were measured using the dietary history, and the outcome was converted into 18 food groups. Factor analysis, for identification of dietary pattern, was carried out, and factor score estimates were produced for each subject, then classified into three classes defined as non-Mediterranean Diet, Prudent (or Intermediate Diet), and Mediterranean Diet. In the factor analysis, the following ratios were found between the class called Mediterranean Diet and that called non-Mediterranean Diet for food groups intake that were critical in the identification of factor score: bread 2.07, cereals 2.6, potatoes 3.80, vegetables 4.21, oils 1.79, fish 3.70, sugar 0.71 and milk 0.40 [19]. These ratios may have practical significance and might be taken into account for practical purposes when giving suggestions to individuals who may be willing to modify favourably their diet for preventive purposes.
Mortality data were classified into three large groups, i.e., major cardiovascular diseases (coronary heart disease, heart disease of uncertain etiology, stroke, peripheral artery disease), all kinds of cancers, and all other causes, plus all-cause mortality.
The role of the three behavioural characteristics in predicting mortality from those few large groups of causes of death is reported in Table 1. The comparison deals with the extreme classes of each behaviour, that is non-smokers versus heavy smokers, vigorous activity versus sedentary activity and Mediterranean Diet versus non-Mediterranean Diet. People who are non-smokers, physically very active or following a Mediterranean Diet are protected against cardiovascular diseases, cancer, other causes and all-cause mortality. This protection is not statistically significant for all other causes and for the relationship of physical activity versus cancer. An intermediate class does exist between each pair of extreme classes, usually carrying an intermediate risk.
Table 1. Italian Rural Areas of the Seven Countries Study: 1,712 men followed up for 50 years. Relationship of entry smoking habits, physical activity and dietary habits with mortality in 50 years derived from Cox proportional hazards models.
|
Causes of death in 50 years (+) |
% of all deaths |
Smoking habits (A) |
Physical activity (B) |
Dietary habits (C) | |
|---|---|---|---|---|---|
|
|
|
Relative risks |
|||
|
Major cardiovascular disease |
43.7 |
0.68 * |
0.63 * |
0.68 * |
|
|
All cancers |
27.6 |
0.65 * |
1.01 |
0.54 * |
|
|
All other causes |
28.7 |
0.86 |
0.80 |
0.77 |
|
|
All causes |
100.0 |
0.72 * |
0.68 * |
0.67 * |
|
A) Non-smokers (including ex-smokers) versus Heavy smokers. B) Vigorous activity versus sedentary activity. C) Mediterranean Diet versus non-Mediterranean Diet. Between each pair of behaviours there is an intermediate group. (+) 1,669 fatal events corresponding to 97.5% of the initial cohort. * Significant p<0.05.
The magnitude of the relative risk states that, depending on the characteristic and cause of death, the protection corresponds to a reduced mortality of between 20 and 46%. Considering all-cause mortality over 50 years, to refrain from smoking corresponds to a reduced mortality of 28%, being physically active to a reduced mortality of 32%, and using a Mediterranean Diet to a reduced mortality of 33%.
Risk reduction can be translated into longer survival, although competing risks may intervene along the way. Survival itself has been analyzed by producing Kaplan-Meier survival curves for all-cause mortality as a function of three classes of each behavioural characteristic (Figure 1). The survival curves are largely separated from each other. The upper curve of each panel corresponds to the healthy behaviour and is associated with a longer survival.
Figure 1. Italian Rural Areas of the Seven Countries Study: 1,712 men followed up for 50 years. Kaplan-Meier survival curves for survival in 50 years, as a function of entry smoking habits, physical activity and dietary habits.
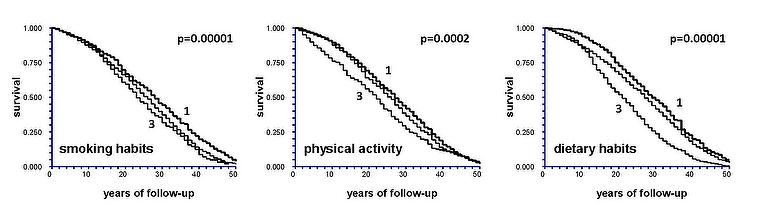
Smoking habits: 1 = non-smokers; intermediate line = moderate smokers; 3 = heavy smokers. Physical activity: 1 = vigorous activity; intermediate line = moderate activity; 3 = sedentary activity. Dietary habits: 1 = Mediterranean Diet; intermediate line = Prudent diet; 3 = non-Mediterranean Diet. p-values represent chi square of log-rank test.
Another way to interpret survival is given by the solution of a multiple linear regression model where the dependent variable is the length of survival (life expectancy), and the independent variables are the behavioural characteristics (Table 2). All behavioural characteristics are statistically significant and beneficial versus the reference class. The magnitude of the coefficients indicates the number of years gained versus the reference of the single behavioural characteristic.
Table 2. Italian Rural Areas of the Seven Countries Study: 1,712 men followed up for 50 years.
Relationship of entry smoking habits, physical activity and dietary habits with life expectancy in 50 years derived from a multiple regression model.
|
Behavioural characteristic |
Coefficient |
Low 95% CI |
High 95% CI |
p |
|---|---|---|---|---|
|
Constant |
74.54 |
69.21 |
79.87 |
0.0000 |
|
Age, years |
-1.15 |
-1.25 |
-1.05 |
0.0000 |
|
Heavy smokers |
reference |
---- |
---- |
---- |
|
Moderate smokers |
2.45 |
0.94 |
3.96 |
0.0015 |
|
Non-smokers |
4.84 |
3.30 |
6.39 |
0.0000 |
|
Sedentary physical activity |
reference |
---- |
---- |
---- |
|
Moderate physical activity |
2.74 |
0.84 |
4.64 |
0.0048 |
|
Vigorous physical activity |
3.88 |
2.18 |
5.59 |
0.0000 |
|
Non-Mediterranean Diet |
reference |
---- |
---- |
---- |
|
Intermediate Diet |
2.53 |
1.25 |
3.82 |
0.0001 |
|
Mediterranean Diet |
4.12 |
2.54 |
5.69 |
0.0000 |
The magnitude of the coefficients indicates the number of years gained versus the reference class of the single behavioural characteristic. CI: confidence interval
In this particular experience, a combination of refraining from smoking, being physically active and adopting a Mediterranean Diet is associated with a 12.8-year longer survival versus those who are heavy smokers, physically sedentary and using a non-Mediterranean diet. In fact, the estimated mean survival for those with three healthy habits was 29.8 years, while it was 17.0 years for those with three unhealthy habits, with an overall mean of 26.3 years during the 50-year follow-up [22].
Interestingly enough, people classified as following a Mediterranean Diet versus those classified as following a non-Mediterranean Diet had lower mean serum cholesterol (14 mg/dl), systolic blood pressure (17 mmHg) and body mass index (4.6 kg/m2), the latter corresponding to about 13 kg.
We have also made separate analyses(not reported here) where further risk factors were tested in addition to the behavioural characteristics reported here, largely independent from the lifestyle behaviours.
CONCLUSIONS
Although factors other than those discussed here, e.g., psychosocial problems, stress, genetic patterns, etc., are contributary, it is clear that behavioural characteristics play an important role in health and disease, survival and death. In accordance with reports from the WHO and another organisation [26,27] it is clear that a global approach to adopting benficial behaviours is merited. Smoking habits have already been targeted with some success. Regular physical exercise is beneficial and should be promoted, especially given the dramatic decline in vigorous physical work. Changing dietary habits may be more of a cultural challenge due to past agriculture and food production, climate and traditions [28]. The adoption of a Mediterranean-style diet (or a parallel choice based on oriental foods) has become an educated choice, partly favoured by the ready availability of a wide variety of fresh foods. However, preventing or postponing one disease may only lead to other severe degenerative diseases intervening with which patients and physicians will have to cope [29,30].
The evidence reviewed and the personal experience reported [22] may help to underline important take-home messages for practising cardiologists.
First of all, among young and middle-aged individuals, it may help to popularize that refraining from smoking habits, being physically active and following a Mediterranean diet (or an equivalent orientally derived diet based on comparable nutritional principles and elements [28]) has a measurable very long-term impact on years of life gained and a sizable effect on preventing the most threatening (among impacting) diseases in society, including cardiovascular diseases and cancers.
Second, paying attention to dietary lifestyle as an effective action for taking preventive measures may easily increase the willingness to adopt healthy foods and, in particular, to avoid those rich in salt and trans fatty acids [9,10]. Moreover, there are other dietary measures that should be followed: reducing sugar intake and increasing a physically active life might combine to keep the intake/expenditure caloric balance and so prevent weight and blood pressure increases (among other favourable effects), further contributing to benefits against cardiovascular and all-cause mortality [31]. Interestingly enough, we have shown here that people following a healthy Mediterranean diet also had 14 md/dl lower mean serum cholesterol, 17 mmHg lower systolic blood pressure and a 13 kg lower body weight.
These targets might be reproduced in clinical practice and there is therefore plenty of room for effective action to improve health and fight the burden of diseases accounting for most deaths [26,27].