
Interestling link: Cardiac Pacing and Resynchronisation therapy guidelines.
The rise in the number of elderly advanced heart failure patients has led to overcrowding of in-office follow-up management and increasing numbers of more performing but also more complex implantable cardiac devices that have added to the problem.
Remote monitoring has helped to reduce the number of visits and allowed for more accurate follow-up and comes as a safe, cost-effective and comfortable alternative to face-to-face follow-up visits, especially useful for post-implant checks, where programming changes are rarely required (1,2,3).
On battery and lead parameters, physicians will access and check for significant electrophysiological events, such as arrhythmias, and review the therapy administered through implantable defibrillator devices (ICDs); in heart failure patients, they will look for transthoracic impedance and patient activity.
As a complement to in-office cardiac device follow-up visits, remote monitoring that has developed and improve since 2001 is feasible, a safe, cost-effective (20) and increases patient and practitioner satisfaction. Remote monitoring for pacemakers, ICDs, cardiac resynchronisation devices and other devices, such as the implantable Holter monitor is available.
I - Systems
Home-monitoring (Biotronik) Germany; no landline necessary, travelling possible: This German system from 2001 uses a portable transmitter that sends information to a GSM network in Germany (Cardio Messenger). No landline telephone is necessary. Continuous day-long monitoring is provided, as is the possibility of transmission while traveling.
Thirty-second electrograms are periodically sent for interpretation by a physician, and different alerts can be configured online.
Significant events can be reported by fax, e-mail or text message in order to ensure optimal follow-up.
Carelink (Medtronic) no landline necessary, only in patient's home country (Europe): This wireless system has been available in Europe since 2005. It requires an analogue landline phone and cannot transmit unless the patient is in his or her home country. One advantage is the automatic testing feature, including automatic atrial, right ventricular and left ventricular capture thresholds, which facilitates full remote follow-up.
Remote visits should be scheduled on line by specialised health practitioners. Practitioners can also adjust different levels of alerts to individual patient characteristics. These alerts are transmitted to the physician by e-mail or text message. Another advantage is its coverage of transthoracic impedance monitoring in patients with dual chamber devices, potentially a useful option in heart failure management.
Latitude (Boston Scientific): landline necessary but travelling possible. This system was first introduced in Europe in 2009. Its transmitter also uses an analogue landline that may be configured for use in more than one country.
Its ability to transmit readings from wireless weight scales and blood pressure cuffs is a useful remote monitoring tool for the management of heart failure patients.
Event notifications can be configured individually, as in the Carelink system, based on different levels according to event severity. Another advantage is its ability to transmit information to different physicians, such as a general cardiologist and a general practitioner, with the resulting benefits in patient management.
Merlin (St Jude Medical) communicates by radio in Europe. The wireless transmitter (Merlin@home) was introduced in Europe in 2008. The system communicates automatically by radio. It uses an analogue landline phone and can be fitted with a cellular adapter. Different events are transmitted to the physician by text message, fax or e-mail. It has the ability to leave reminders of in-office visits on the patient’s transmitter and to make automatic phone calls reporting that all parameters are normal (4 Europace 2009).
II - What to check for at visits
Most ICD monitoring systems feature these measures :
- Type of event, necessity of therapy, only monitored event
- Daily activity
- Percentage of stimulation and sensing if different chambers are available
- Stimulation mode, amplitude of impulse
- Voltage, capacitor, charge time of battery. Impedance, stimulation and defibrillation of leads. Thresholds of sensed wave amplitude.
1 - Lead dysfunction
The lead system is an important component of all implantable devices. However, its complex electrodes are susceptible to defects, fractures, exposing patients to the risks of inappropriate therapy and failure of defibrillation when necessary or loss of pacing.
Adverse clinical events related to lead dysfunction may be preceded by asymptomatic abnormal electrode characteristics, such as impaired lead impedance, oversensing of non-cardiac potentials or inappropriate increase in pacing rate.
Remote monitoring can contribute to a prior diagnosis of lead dysfunction that can potentially avoid adverse events related to electrode fracture or dislodgement (5).
Fig. 1: Recording from a Biotronik ICD (Home Monitoring system) device showing low amplitude of right ventricle R wave which could be related to lead dysfunction.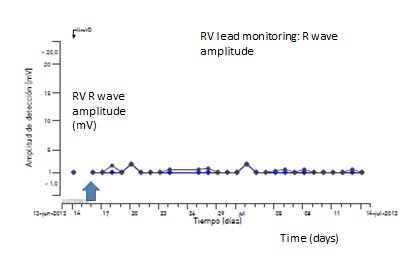
2 - Atrial arrhythmias or subclinical atrial tachyarrhythmias
Clinical atrial fibrillation is a common arrhythmia responsible for 15% of ischemic strokes, however, in about 25% of such events no evident cause is detected. These are presumably related to non-clinical atrial fibrillation. When a lead is implanted in the atrium, asymptomatic episodes of atrial arrhythmias can be detected.
Recently Healey et al. showed that in patients with cardiac devices and no clinical atrial fibrillation, subclinical atrial tachycardia was associated with an increased risk of ischemic stroke and concluded that subclinical atrial tachyarrhythmias often precede clinical atrial fibrillation.
Routine use of remote monitoring systems could be useful for prior detection of silent episodes such as these, enabling the physician to start oral anticoagulation if indicated and to avoid thromboembolic events (6, 7, 8).
Atrial arrhythmias may often go undetected (figure 2). Thus, a careful examination of electrograms is mandatory when revisions are performed remotely.
Fig. 2.
Panel A: Episode of silent atrial fibrillation detected by an ICD device.
Panel B: Atrial tachycardia episode recorded, but not detected by a CRT-D device. Note that atrial activity (arrow) is regular, probably a typical atrial flutter, cycle length 200 msec. 
ICD: implantable cardiodefibrillator). CRT-D: cardiac resynchronisation therapy with defibrillator.
3 - Ventricular tachycardia
The main use of ICDs is to detect and treat potentially fatal ventricular arrhythmias in selected patients according to current guidelines (9, 10, 11).
ICDs are promptly revised post implant and furthermore every three to six months, according to individual center availability (4).
Nielsen et al. (12) published a prospective study of patients with a Biotronik ICD and Home Monitoring system with a mean follow-up of 10 months. At least one relevant event occurred in 41% of patients, mostly potentially lethal arrhythmias. Around 60% of these events occurred during the first month after the last in-office visit.
Another study enrolling about 11,000 patients showed that the mean interval between the last face-to-face visit and a remote monitor-notified event was 26 days. That means a gain of 154 days compared with a six-month follow-up routine, and 64 days compared to a three-month follow-up routine (13).
The results of these studies suggest the usefulness of a remote monitoring system for prior detection of clinically relevant events such as ventricular arrhythmias. Examples of different therapies are shown in figure 3.
Fig.3:
Panel A: Electrogram from a Medtronic ICD device obtained by Carelink system. Note the initial presence of ventricular tachycardia and non-effective anti-tachycardia pacing (blue arrow). Red arrow marks the persistence of a modified ventricular tachycardia after pacing.
Panel B: Continuation of ventricular tachyarrhythmia (green arrow), terminated by an effective shock. 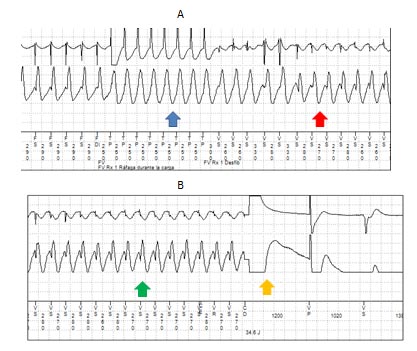
III - Therapies
1 - Avoiding inappropriate ones.
An ICD carrier has an increased risk for anxiety and depression disorders, mostly because of the shocks administered by the device.
Therefore, avoiding inappropriate therapies in patients with cardiac devices may be a priority for the treating physician (14).
A remote monitoring system could be useful for detecting lead dysfunction (such as dislodgement or fracture) or rapid atrial arrhythmias that could develop into inappropriate shocks. Examples of inappropriate therapies are shown in figure 4.
Fig. 4:
Panel A: Episode of rapid atrial fibrillation (red arrow) and inappropriate antitachycardia pacing (blue arrow).
Panel B: Inappropriate shock (blue arrow) in a patient with rapid atrial fibrillation. Register from a Medtronic ICD device obtained by Carelink remote monitoring system.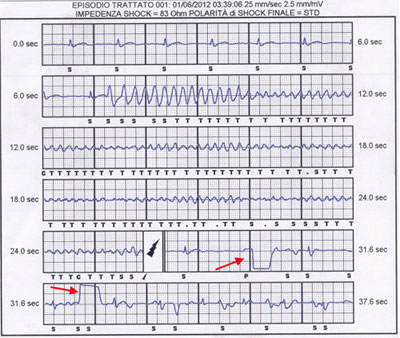
2 - Cardiac resynchronisation follow-up
Following up cardiac resynchronisation devices is challenging due the complexity of the device and the patient’s heart disease. Several potential causes of heart failure instability can develop into hospital admission or cardiovascular death.
Added to the usual parameters reviewed above, certain remote monitoring systems offer additional measures, such as transthoracic impedance, physical activity, body weight or special alerts according to symptoms. Special attention should be payed by physicians to events such as:
- Atrial arrhythmias
- Ventricular arrhythmias
- Transthoracic impedance disorders (Fig. 5)
- Low physical activity
- Electrode disorders
- Symptoms triggering transmissions
Several studies have shown how prior detection of these events is possible with a remote monitoring system (15, 16).
In 2012, Landolina et al. suggested that, compared with the usual practice, a proper remote monitoring strategy could reduce the number of emergency department visits (17).
Indeed, the 2012 EHRA expert consensus on cardiac resynchronisation therapy includes remote follow-up visits in addition to clinic follow-ups, and it encourages patients to transmit if changes in symptoms appear (18).
IV - Recommendations
Below are the recommendations offered by the European heart failure association in its expert document regarding pacemakers, ICDs and CRT(19):
- First revision within 72 hours of implantation (in-office)
- 2-12 weeks after implantation (in-office)
- Every 3-12 months, pacemaker/CRT-P (cardiac resynchronisation therapy pacemaker) (in-office or remote monitoring)
- Every 3-6 months, ICD/CRT-D (in-office or remote monitoring)
- Yearly until battery depletion (in-office)
- Every 1-3 months if evidence of battery depletion (in-office or remote monitoring)
Conclusions
Remote monitoring offers detection of adverse events even before symptoms appear. The physician is able to check most of the parameters recommended in the consensus document for proper device follow-up. The treating physician must search carefully for arrhythmic events and lead dysfunction.
Prior detection of silent atrial arrhythmias offers the possibility of oral anticoagulation initiation in order to prevent ischemic strokes.
Inappropriate ICD therapies are undesirable adverse events that have an important psychological impact on patients and can be detected by remote monitoring, for prompt management by the treating physician.
Cardiac resynchronisation devices need special attention due to their complexity and due to the severity of the underlying cardiac disease.
The expert consensus recommends remote monitoring as a valid complement to in-office visits.
Further studies are needed in this field before remote monitoring is recommended as a complete alternative to physical follow-ups.