
Background
Pericarditis is an inflammation of the pericardial sac, a fibroelastic structure that usually contains 15-50 ml of plasma ultrafiltrate. A congenitally absent pericardium or pericardial cysts are uncommon structural abnormalities that are usually asymptomatic whereas pericardial effusion, cardiac tamponade, constrictive pericarditis and acute pericarditis are forms of pericardial disease that are symptomatic.
Moreover, patients affected by pericarditis can subsequently develop chronic or recurrent pericarditis, which is difficult to prevent. This article reviews the latest on diagnosis, treatment and follow up of acute pericarditis.
I - Diagnosis
Pericardial disease can occur as an isolated entity - typically pericarditis, or a manifestation of a systemic disorder stemming from inflammatory diseases such as systemic lupus erythematosus, rheumatoid arthritis or cancer (1).
Many cases of acute pericarditis are presumed to be viral in aetiology: viruses involved are echovirus and coxsackievirus A and B. They may even be cytomegalovirus, influenza-, adeno- and herpes viruses or HIV - testing for specific viruses is not routine practice because determining the virus rarely has an impact on treatment. Furthermore, this process is expensive.
Acute idiopathic pericarditis usually affects young and otherwise healthy individuals. Many patients have mild symptoms, don’t seek medical help and the conditions resolve on their own. It is estimated that 80-90% of all cases of acute pericarditis are presumed to be idiopathic.
An early set of symptoms - a prodrome - of fever (usually <39°C), malaise and myalgia and/or arthralgia is common. The typical complaint is chest pain, that is most often pleuritic (exacerbated by inspiration). Patients may note lessening of the pain when they lean forward or are in the upright position. The most difficult differential diagnosis is myocardial infarction (MI). As in MI, chest pain can radiate to the neck, arms, or left shoulder; however, if pain radiates to one or both trapezius muscle ridges it is likely due to pericarditis because the phrenic nerve that innervates these muscles traverses the pericardium.
Physical examination will uncover an audible friction rub, which is highly specific for pericarditis: it is present in 85% of patients at some time during the course of the disease. It is usually a high-pitched, scratchy or squeaky sound best heard at the left sternal border and consisting of 3 phases that correspond to the movement of the heart during 3 phases of the cardiac cycle: 1) atrial systole, 2) ventricular systole, and 3) rapid ventricular filling during early diastole. However, some rubs are present in only one (monophasic) or two (biphasic) components of the cardiac cycle (2).
The electrocardiogram (ECG) is the most important tool in the diagnosis of pericarditis. It may show sinustachycardia and widespread ST-segment elevation which has been considered the hallmark of acute pericarditis. Nevertheless the pericardium is electrically silent. Indeed, the ST-elevation is the expression of subepicardial myocardial involvement and has been reported in 60% to 90% of consecutive cases of acute pericarditis, while troponin elevation has been reported in a higher number of cases yet (90–98%). Thus, mixed myocardial and pericardial involvement is probably present in the majority of cases (3).
The ST segment is usually coved upward and resembles the current of injury of acute transmural ischemia. The distinction between acute pericarditis and ischemia is not usually difficult because lead involvement is more extensive in pericarditis and prominent reciprocal ST-segment depression in ischemia, which usually is absent in pericarditis, shows. Another recent criteria to differentiate acute STEMI from acute pericarditis may improve the differential diagnostic yield of the classical ECG criteria; it is the prolongation of the QRS complex and shortening of the QT interval in ECG leads with ST segment elevation which are not the case in patients with pericarditis (4) (Figure 1).
PR-depression is another feature in the ECG of the patient with pericarditis. According to a study by Porela et al the most common location for PR depression was lead II (55.9%), while this ECG finding least likely appeared in lead aVL (2.9%). PR depression in any lead had a high sensitivity (88.2%), but fairly low specificity (78.3%) for myopericarditis. The combination of PR depressions in both precordial and limb leads had the most favourable predictive power to differentiate myopericarditis from STEMI (positive 96.7% and negative power 90%) (5).
Other mandatory checks besides auscultation and ECG according to the latest European guidelines on pericardial diseases are echocardiography to rule out effusion, concomitant heart disease or signs of myocarditis, blood work for inflammation markers and myocardial enzymes, and chest X-ray, for differential diagnostic purposes especially. (See Table 1) (6)
II - Treatment
Patients with pericarditis can be safely managed on an outpatient basis without a thorough diagnostic evaluation unless a specific cause is suspected or in a case of high-risk features, or both. A targeted aetiological search should be directed to the most common cause on the basis of clinical background, epidemiological issues or specific presentations. In developed countries clinicians should rule out pericarditis related to a systemic disease as well as neoplastic, tuberculous, and purulent pericarditis (7).
Hospitalisation in acute pericarditis is usually not necessary unless the clinical picture suggests non-idiopathic causes or a hemodynamically compromised patient. Fever >38°C (>100.4°F), subacute development of symptoms (characteristic of tuberculosis, neoplastic disease, uremia, or collagen vascular disorders), hypotension, jugular venous distension, a large pericardial effusion, or echocardiographic features of impending tamponade may warrant hospitalisation. Patients who are immunocompromised or anticoagulated should also be observed initially in the hospital (8).
Treatment is directed to resolving symptoms. Non-steroidal anti-inflammatory drugs (NSAID) being the mainstay (level of evidence B, class I). Ibuprofen is preferred for its fewest side effects (and favourable effect on coronary blood flow). Depending on severity and response, 300-800 mg every 6-8 hrs may be initially required and can be continued for days or up to a couple of weeks. Gastrointestinal protection must be provided in all patients.Colchicine (0,5 mg bid) added to an NSAID or as monotherapy is also effective and has been shown to prevent recurrences (level of evidence B, class IIa indication). Systemic steroid therapy (prednisone 1mg/kg/day for at least one month) is restricted to patients with symptoms refractory to standard therapy or to other forms of non-idiopathic pericarditis such as uremic pericarditis or pericarditis secondary to connective tissue diseases. A common mistake is to use a dose too low to be effective or to taper the dose off too rapidly. For tapering of prednisone, ibuprofen or colchicine should be introduced early (class IIa, level of evidence B). Patients with acute pericarditis have a good prognosis in general but are prone in some degree to recurrences, especially during viral infections.
Conclusions
Patients with acute pericarditis should avoid strenuous activities as long as symptoms persist. Some advocate assessment of CRP at presentation and then weekly, with anti-inflammatory drugs prescribed until complete resolution of symptoms and normalisation of CRP (9). The acute stage lasts usually from days to a couple of weeks. No recommendations have been issued regarding short term follow up of these patients although some local routines include an exercise stress test and/or echocardiography 6 weeks after resolution especially in young and/or active individuals.
Figure 1: Echocardiography of the acute stage of pericarditis.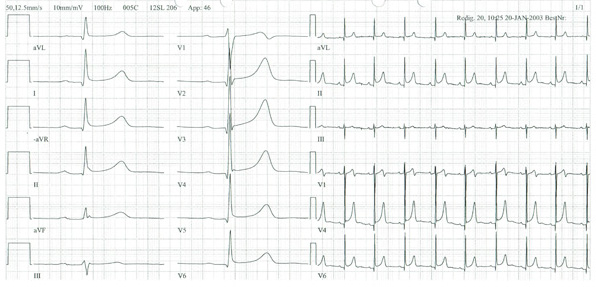
Table 1: Diagnostic pathway and sequence of performance in acute pericarditis (level of evidence B for all procedures). (6)
| Technique Obligatory (indication class I) |
Characteristic findings |
| Auscultation | Pericardial rub (mono-, bi-, or triphasic) |
| ECG | Stage I: anterior and inferior concave ST segment elevation. PR segment deviations opposite to P polarity Early stage II: ST junctions return to the baseline, PR deviated Late stage II: T waves progressively flatten and invert Stage III: generalised T wave inversions Stage IV: ECG returns to prepericarditis state |
| Echocardiography | Effusion types B–D (Horowitz) Signs of tamponade |
| Blood analyses | (a) ESR, CRP, LDH, leukocytes (inflammation markers) (b) Troponin I, CK-MB (markers of myocardial lesion) |
| Chest X-ray | Ranging from normal to “water bottle” heart shadow. Revealing additional pulmonary/mediastinal pathology |