

Background
Since the introduction of coronary artery bypass surgery (CABG) in 1968 and percutaneous transluminal coronary angioplasty (PTCA) as a nonsurgical alternative in 1977 - with bare-metal (1987) and then drug-eluting stents (1991) broadening the range of acts performed on the lumen and PTCA becoming part of the broader term percutaneous coronary intervention (PCI) - both CABG and PCI remain an option in a large part of patients with coronary artery disease today (1).
Nevertheless, cardiovascular variability of PCI-to-CABG from one country/center to another is high and raises concerns over inappropriate revascularisation and elected procedure.
Leaving aside varying economic considerations and expanded PCI indications, many decisions are case-by-case and surgeons and cardiologists can differ in the information they give regarding the choice between PCI and CABG and PCI to patients resulting in PCI to be overly used on the whole (2).
There is also growing awareness that a multidisciplinary approach to medicine, as seen in tumor boards or organ-approach centers, improves level of care where physicians work together and thus avoid one individual physician-related factors driving treatment.
Indeed, patient centric evidence-based care multidisciplinary Heart Teams would probably offer the best care to patients (3).
For example, in trans-aortic valve implantation, a heart-team approach decided which maneuvres to attempt in complications resulted in better survival than when physicians decided on strategies on their own (4).
Risk scores also play an important part in deciding on the optimal strategy. While they are important in the decision-making process - the 2009 perioperative guidelines as well as the 2010 guidelines on myocardial revascularisation state that risk scoring as the first of its take home message, they should only be used as a guide. After describing the history of the Heart Team concept, its advantages and limitations, we describe how to use risk scores to the Heart Team's advantage.
I - Heart Team
Guidelines
The heart team approach can be found in the SYNTAX trial (2008) as a means to select and randomise the patients according to their coronary lesions (1). It was an all-comers trial including 1,800 patients with three-vessel disease, left main disease or LM equivalent with or without 1, 2 or 3 diseased vessels, de novo lesions with at least 50% stenosis and myocardial ischemia. The Heart Team was designed as a 1) heart surgeon and 2) an interventional cardiologist and both reviewed each clinical case. Consensus agreement was obtained as to which procedure(s) the patient was eligible for – CABG or PCI.
In 2010, the ESC took this approach into its guidelines on myocardial revascularisation (2010) (5) and wrote about the concept of the Heart Team jointly with the European Association for Cardio-Thoracic surgery. The guidelines state that revascularisation strategy should be based on best evidence and discussed on a multidisciplinary level, within a Heart Team, that will require interaction between 1) cardiologists and 2) cardiac surgeons, 3) referring physicians or other specialists as desirable - as anaesthesiologists, geriatricians, or intensivists.
The ACCF/AHA guideline for CABG (6) and one for PCI (7) (2011) followed up as well to recommend a Heart Team approach, defined as a multidisciplinary approach for revascularisation, made up of an 1) interventional cardiologist, 2) a cardiac surgeon, and often 3) the patient’s general cardiologist in patients with unprotected left main or complex CAD.
The latest ESC guidelines in valvular heart disease recommend that decision-making in patients with valvular disease should be driven by a ‘‘heart team’’ with particular expertise in valvular heart disease (VHD), including cardiologists, cardiac surgeons, imaging specialists, anaesthetists and, if needed, other specialists. (8)
Prior evidence
Prior to the above mentioned guidelines, trials and a prior guideline had prefigured the Heart Team.
- The Emory Angioplasty versus Surgery Trial (1997) (9)(EAST) improved survival in the registry may be due to treatment selection. Physician judgment, even in patients judged appropriate for clinical trials, remains a potentially important predictor of outcomes.
- The BARI trial (10) (2000) involving 4,039 patients with multivessel coronary artery disease; 1,829 consented to randomization, 2,010 did not but were followed up in a registry. Physician-guided versus random assignment of PTCA versus CABG proved superior for PTCA.
- ESC perioperative cardiac care (2009)(11) had issued that the timing and type of preoperative coronary intervention options should be discussed with the treating surgeon and anaesthesiologist (as anti-platelet therapy influences perioperative management).
Advantages (2,3)
- Ad hoc intervention: a heart team might be able to establish when it is appropriate to proceed with percutaneous revascularisation following a diagnostic catheterisation or coronary angiogram, while the patient is still on the table and when the procedure be terminated after the angiography so that the surgeon and interventionalist can discuss how to proceed with that patient.
- Informed consent: In order to make a decision the physician must 1) assess the anatomy and function of the heart 2) and the co morbidity of the patient 3) in order to classify the global risk and the specific risk for each method, surgery or coronary intervention. Once a strategy has been defined, the information should be delivered to the patient who can make his or her decision. This process would therefore not be looked at solely as a necessary legal requirement but should be used as an opportunity to optimise objective decision making.
- Sharing the burden and tracking complexity: Involvement in a heart team, although it does not remove responsibilites, can help limit a physician's personal malpractice exposure, and also help track the decision-making process. With patients also more informed, a heart team can also help in trial recruitment.
Limitations
The concept of choosing one treatment over another is organised around the concept of the heart team which involves various physicians such as cardiac surgeons, interventional cardiologist, general cardiologists as well as intensivists. However, much criticism has risen regarding the role of the heart team or on the impact of recent guidelines recommending the heart team approach on a daily routine. Reasons we have observed for not implementing a heart team in the cardiologists decisions include:
- Geographical distance between surgical and angiographic units
- Inability of creating a well cooperating heart team
- Lack of time to cooperate with other specialties
- Cost reimbursement issues
- Simple straightforward cases can be treated ad hoc without requiring the approval of the heart team
- Personal issues related to the different specialists involved in a heart team
- Absence of a cardiac surgery program on site
II - Risk Scores
While finding solutions to the above mentioned hindrances will require time and effort on all parts, risk models are readily available to physicians, interventional cardiologists and cardiac surgeons and can help to ensure that their patients are able to weigh the individual benefits and risks of medical therapy, PCI, and CABG, and come to their own informed decision.
The Syntax score: for evaluation risk of PCI especially
High risk in PCI is characterised more by lesion complexity than co-morbidities, and is therefore best assessed by risks models of angiographic characteristics such as the SYNTAX score.
The SYNTAX score is derived only from the coronary anatomy and lesion characteristics, and is calculated using dedicated software, enabling complex coronary artery anatomy to be quantified (12). It is able to predict 3-year outcomes in patients who have complex coronary artery disease (triple vessel and/or left-main stem) (13). The higher the score, the more the team should turn to CABG.
Amongst patients having CABG both retrospective and prospective studies have concluded, as expected, that the SYNTAX score is a poor predictor of events in patients with complex coronary disease undergoing CABG (14, 15).
Limitations of the SYNTAX score are the absence of clinical variables and the subjective nature of assessment which can lead to inter-observer variability and the absence of SYNTAX score algorithms for the increasing numbers of patients with prior revascularisation (PCI/CABG) who return for secondary revascularization with PCI. (4).
However, the recently published on SYNTAX II score added eight clinical variables (predictors) to its scoring process: anatomical SYNTAX score, age, creatinine clearance, left ventricular ejection fraction, presence of unprotected left main coronary artery disease, peripheral vascular disease, female sex, and chronic obstructive pulmonary disease.
Anatomical and clinical characteristics are thus included into scoring to guide decision making between coronary artery bypass surgery and percutaneous coronary intervention for individual patients, and is able to predict 4-year outcomes (16).
Flow reserve
The FAME study established that utilising flow reserve (FFR) measurements - FFR = Pd/Pa (Pd = pressure distal to the lesion, Pa = pressure proximal to the lesion) - to determine the functional significance of individual coronary lesions and guide subsequent coronary intervention, leads to a potential prognostic impact when compared with angioplasty guidance alone (17, 18).
ACEF score
The ACEF Score is risk model for predicting operative risk in patients undergoing elective CABG uses just three variables: 1) patient’s age, 2) left ventricular ejection fraction and 3) creatinine in the formula: age (years)/ejection fraction (%) +1 (if creatinine>2mg/dl). So far, validation has only been performed in elective patients, where the score was shown to have similar sensitivity/specificity, and similar positive/negative predictive values compared to other risk models including the additive/logistic Euro SCORE (19).
STS score
Society of Thoracic Surgeons (STS) Score: The STS risk model predicts the risk of operative mortality and morbidity after adult cardiac surgery based on patient demographic and clinical variables. It is very comprehensive and includes over 40 pre-operative variables. Since the score was first introduced, it has undergone periodic revision; validation of the current version demonstrates ability to predict mortality with a C-index of 0.812. In addition, when patients are grouped into categories of predicted risk, the absolute difference between the observed and expected event rates is less than 1.5% (20,21).Euro SCORE: for evaluating risk of CABG especially
In patients considered for CABG, high risk is not signaled by lesion complexity, but by multiple co-morbidities. These are best assessed by risk scores that consider patient characteristics. The European System for Cardiac Operative Risk Evaluation (Euro SCORE) is a simple additive bed-side score, calculated using 17 different clinical variables. It has been used since 1999 to predict in-hospital mortality in patients undergoing cardiac surgery (22). The logistic Euro SCORE which requires a calculator, was introduced following validation studies which suggested that the additive Euro SCORE underestimated risk in those at highest risk (23). More recently it has been suggested that this also requires recalibration as it appears to over-estimate risk by a factor of 2-3, which is the likely consequence of it being based on surgical results obtained during the 1990s (24).The potential of the Euro SCORE to risk stratify patients undergoing PCI has been assessed in two prospective, single centre non-randomised studies (25, 26). Its role in the assessment of patients getting CABG is undisputed; whilst, its role in the risk stratification of patients undergoing PCI still requires further evaluation. Several parameters in the score have no relevance for PCI, and therefore modifications to the score are required before it can be fully adopted as a risk model in PCI.
Limitations, and global risk : combining Syntax and Euro SCORE
Risk models should not be relied upon to determine an individual patients' actual risk, but instead should be used as a guide to help make more informed clinical decisions. Physician experience is often one of the most important factors in the final decision, which should always be made at a multidisciplinary level.
The Heart Team approach to assessing a global risk classification would be to combine the Syntax and the Euro SCORE. This approach of global risk classification should allow physicians to better select the appropriate revascularisation strategy. Indeed, a simple graph can be constructed based on the guidelines' recommendations (Fig. 1) combining:
- The anatomy score as defined by the SYNTAX score; low risk being < 23; intermediate 23-32; high risk ≥ 33, and
- The risk score calculated with the Euro SCORE (20) with low risk < 3; intermediate 3-5; high risk > 6.
The more complex the coronary anatomy the more CABG has been shown to improve survival and therefore it is the preferred theoretical treatment choice (5, 6). However, the risk score of the patient should be nevertheless be assessed.
For a high surgical risk, other options such as PCI or medical treatment or incomplete revascularisation - off pump left internal mammary artery to left anterior descending artery (LIMA LAD) bypass - or hybrid strategy should be discussed.
This course allows providing a risk/benefit analysis for an individual patient. Additionally, the need for a given patient may differ according to its lifestyle. Incorporating functional SYNTAX II score may also serve to implement this strategy, as it should be tested in future studies.
Figure 1. Current coronary revascularisation according to risk score and anatomical risk.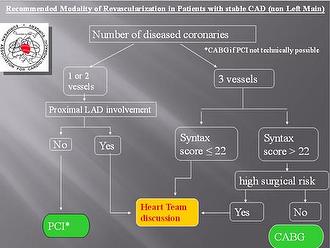
SIHD: stable ischemic heart disease
CABG: Coronary arteries bypass grafting
PCI: percutaneous coronary intervention
Anatomy High risk: Syntax ≥ 33, Intermediate risk: Syntax 23-32, Low risk: Syntax 0-22
Risk score; low risk Euro SCORE < 3; intermediate ES 3-5; high risk ES > 6
Figure 2. Heart team recommendation for coronary revascularisation according to risk score and anatomical risk.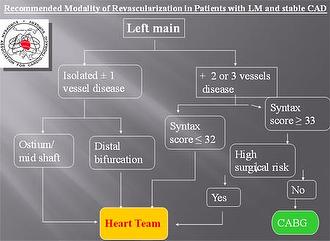
SIHD: stable ischemic heart disease CABG: Coronary arteries bypass grafting PCI: percutaneous coronary intervention
Anatomy High risk: Syntax ≥ 33 Anatomy Intermediate risk: Syntax 23-32 Anatomy Low risk: Syntax 0-22 Risk score; low risk Euro SCORE < 3;intermediate ES 3-5; high risk ES > 6
Conclusions
The guidelines on myocardial revascularisation were the fruit of surgeons' and interventionalists'/cardiologists' societies, mirroring the "heart-team" approach to coronary revascularisation decisions recommended in the guidelines.
Indeed, it was recognised that coronary artery disease decisions on a general recommendation level are best addressed by both associations.
Individual CAD decisions can be complicated and selection of optimal treatment primarily depends on both the complexity of coronary anatomy and comorbidity of the patient therefore use of risk scores can also help with decision-making - the model combining the Syntax and Euroscore that we present being very useful.
Heart teams may also decide to develop local-based protocols. The Heart Team will then be best able to adequately inform patients regarding mortality, stroke, myocardial infarction and angina as well as recovery time, medication and expected lifestyle after each procedure.
Although the Heart Team approach receives the highest level of recommendation (I) it only receives a C level of evidence because heart team decision making needs to be the object of randomised controlled trials: data on heart teams for patients with CAD should build in the next few years.
Distancing us from turf battles and professional silos between specialties we might ease into a Heart Team approach, and perhaps move on to implement Hybrid teams or rooms in the future, where interventionalists and surgeons work in common.