Incidence of atrial fibrillation per 1000 person-years is 3.1 and 1.9 in 64-year-old men and women respectively, 19.2 in the 65-74 age bracket, and 31.4 in the over 80 population, which in Europe, roughly equates to six million and three and a half in the US, and figures are expected to rise as the population continues to age (1,2,3). Sixty percent of these have a permanent form of it, and forty per cent of these patients display severe symptoms, patients with uncontrolled congestive heart failure included.
The initial challenge is to properly detect patients who could benefit from AV junction ablation and pacing. In a prospective, observational, transversal study on the management of AF as primary diagnosis in Italy, we enrolled consecutive in- and out-patients referred to 43 different cardiology departments (4). Although it was observed that atrioventricular (AV) junction ablation and pace-maker implantation had been indicated in 8.6% of patients according to class I indication of Italian guidelines (5) only 2.7% were recommended the intervention by the attending cardiologist. Study results reflect the portion of the physician body who might not refer for intervention because they consider that AV junction ablation merely a palliative or even a potentially harmful.
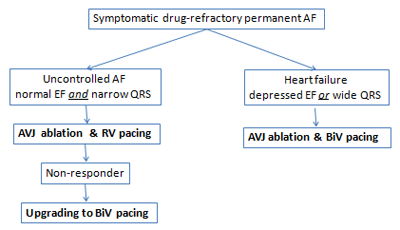
According to guidelines (5), the patients candidates to AV junction ablation are those who: 1) due to high and irregular ventricular rate, had severe symptoms of palpitations, fatigue and shortness of breath during physical activity and at rest with chest discomfort greatly impairing quality of life; Or 2) having a CRT indication due to drug-refractory heart failure, depressed left ventricular (LV) function and wide QRS complexes, have the need to avoid competitive atrial rhythm in order to assure a constant biventricular pacing
In fact, randomised observational studies from the last two decades having enrolled in total over a thousand patients have shown that, AV junction ablation and permanent pacing from the RV apex provide efficient rate control, regularisation of AF and improve symptoms without deterioration of the ventricular function (6-13). In a recent sub-analysis of the APAF trial (14), when compared with the pre-ablation evaluation in quality of life scores, great improvement in exercise capacity and cardiac performance was observed at 6 months (Table 1).
However, AV junction ablation and permanent right ventricular (RV) pacing cause a non-physiologic asynchronous contraction which might partly counteract any beneficial effects of ablation. Indeed, right ventricular pacing induces a ventricular activation sequence resembling that of left bundle branch block, i.e. the right ventricle is activated before the left, thus causing inter-ventricular dyssynchrony. Likewise, the LV septum is activated before the LV free wall causing intraventricular dyssynchrony. Resynchronisation therapy (CRT) achieved through AV junction ablation can restore proper synchrony.
In a sub-analysis on 171 patients of the recent APAF trial (14), 63% of patients had improved clinical conditions, 9% had no change and 28 % worsened with RV pacing during a median follow-up of 20 months. With biventricular pacing however, 83% improved, 5% had no change and 12 % had a worsened clinical condition (p=0.001 versus RV pacing). Furthermore, beneficial effects from CRT were consistent in patients who met the current recommendations from expert consensus for CRT, ejection fraction ≤35%, NYHA class ≥III and QRS width ≥120, (class IIa, level of evidence B), as well as in those who did not. In patients affected by severely symptomatic permanent AF, patients had a greater benefit from AV junction ablation and CRT pacing than RV-paced patients irrespective of the severity of the underlying structural heart disease and of current guidelines criteria. After multivariable analysis, only the CRT mode remained an independent predictor of clinical benefit (p=0.001).
As no clinical difference was observed in the outcome of patients treated with biventricular pacing who met the current guideline indications, with those who did not, the results from the APAF study suggest that the indications for CRT should be extended to all patients with severely symptomatic AF undergoing AV junction ablation.
Nevertheless, considering the higher costs and complications of CRT, an alternative strategy of CRT upgrading may be a reasonable clinical option in patients who, for any reason, were initially paced at the RV only. “Upgrading” to BiV pacing in patients who developed heart failure months or years after AV junction ablation resulted in a clinical benefit similar to that of “de-novo” CRT pacing (16,17,18). Leon et al (16) had upgraded 20 patients who became severely symptomatic 17 months after AV junction ablation and RV pacing to BiV pacing; they observed an improvement of NYHA class of 29%, of Minnesota LHFQ score of 33% and a reduction of hospitalisation of 81%. Similar results were obtained more recently by Valls-Bertault V et al and by Frohlich G et al (17, 18). In the 2011 APAF sub-analysis (14), upgrade was performed in 14 patients who had developed “clinical failure” after a median of 12 months of RV pacing (Table 2); after 3 months, these patients showed a significant reduction in specific AF symptoms and an improvement in cardiac performance similar to that observed in “de novo” CRT pacing shown in Table 1.
Table 1. Changes between baseline and 6-month follow-up after AV junction ablation in 158 patients.
| Endpoint | Baseline | 6th month | P value | % difference |
|---|---|---|---|---|
| New York Heart Association class | 2.5±0.6 | 2.1±0.7 | 0.0001 | -16% |
| Minnesota LHFQ, score (b) | 40±19 | 26±20 | 0.0001 | -35% |
| 6 min walking distance, meters | 322±123 | 348±134 | 0.01 | +8% |
| Endpoint | Baseline | 6th month | P value | % difference |
|---|---|---|---|---|
| Specific Symptom Scale, score (c) | ||||
| 1-Palpitations | 4.5±3.2 | 1.3±2.2 | 0.0001 | - 71% |
| 2-Effort dyspnea | 6.1±3.1 | 3.5±3.1 | 0.0001 | - 43% |
| 3-Rest dyspnea | 2.7±2.8 | 1.3±2.3 | 0.0001 | -52% |
| 4-Exercise intolerance | 5.7±3.2 | 3.9±3.2 | 0.0001 | -32% |
| 5-Easy fatigue | 3.1±3.1 | 1.4±2.4 | 0.0001 | -55% |
| 6-Chest discomfort | 1.6±2.5 | 0.6±1.8 | 0.0003 | -63% |
| Total score | 24±13 | 12±11 | 0.0001 | -50% |
| Endpoint | Baseline | 6th month | P value | % difference |
|---|---|---|---|---|
| Echocardiogram, mean (SD) | ||||
| Ejection fraction,% | 38±14 | 44±15 | 0.001 | +16% |
| LV end-diastolic diameter, mm | 60±10 | 59±10 | 0.30 | -2% |
| LV end-systolic diameter | mm 46±11 | 43±12 | 0.02 | -7 % |
Minnesota LHFQ (Minnesota Living With Heart Failure Questionnaire) scores range from 0 to 105 higher scores indicating worse health status
Specific Symptom Scalescores range from 0 to 60 (total score) each item ranging from 0 to 10, higher scores indicating worse health status.
Conclusion:
Our current decision-making algorithm used in clinical practice is summarised in Figure 1.
Figure 1: AV junction ablation and pacemaker therapy in patients with permanent AF