

1. Definition
Obesity is progressively becoming a major, world-wide threat to health. Due to its increasing prevalence in almost all countries, obesity is considered an epidemic, especially in developed countries. Overweight is also the most prevalent cardiovascular risk factor in patients with established coronary heart disease (1,2).
Obese individuals have both a worsened quality of life and shorter life expectancy than normal-weight individuals. Epidemiological studies have shown that obesity is a major risk factor for most severe cardiovascular outcomes, including coronary heart disease, heart failure, atrial fibrillation, ventricular arrhythmias, and sudden death. It is also considered a causal factor in hypertension, type 2 diabetes mellitus, osteoarthritis, obstructive sleep apnea, dyslipidemia, gastroesophageal reflux, non-alcoholic fatty liver disease and many forms of cancer.
Multiple disease mechanisms are involved in cardiovascular diseases related to obesity: subclinical inflammation, endothelial dysfunction, increased sympathetic tone, atherogenic lipid profiles, enhanced thrombogenic factors, obstructive sleep apnea, etc.
Body mass index (BMI) is widely used as a surrogate measure of obesity (Table 1) (3). Many investigators acknowledge that BMI can underestimate the true prevalence of obesity, if defined as an excess of body fat content. Gómez-Ambrosi J et al (4) have recently shown an excellent correlation between body fat percentage (BF%) and glucose disorders even in subjects with normal BMI.
2. Treatment
2.1. Lifestyle modifications
Lifestyle changes are the initial and basic steps in all obese patients. The improvement of most of the abnormal metabolic correlates of obesity and metabolic syndrome can be obtained through deep changes in daily activity and dietary habits. In the Diabetic Prevention Program, a lifestyle modification program obtained a significant delay in the onset of diabetes (5), and a significant reduction in the incidence of other cardiovascular risk factors such as dyslipidemia and hypertension.
Current guidelines recommend dietary intervention and frequent physical activity for the prevention and treatment of overweight (6). They also consider an adjustment of daily calorie intake with respect to energetic needs (known as negative energetic balance, mandatory. There are many types of calorie restriction patterns (low carbohydrate, low protein or low fat diets); their effects on cardiovascular risk are probably due to their effects on cardiovascular risk factors (7). Many important studies have confirmed that despite the same amount of physical activity, the reduction in calorie intake will translate into weight loss, independently from the predominant macronutrients content of the diet (carbohydrates, fat or proteins). Diets that are extremely restrictive in carbohydrates (Atkins, Duncan, etc), obtain more weight loss in the initial 6 weeks than low fat diets, but not in the long-term. Additionally, this type of calorie restriction has raised security concerns in the long-term and due to their restriction in the amount of vegetables and whole grains, regarding benefits in terms of global cardiovascular risk.
Physical inactivity is an endemic cardiovascular risk factor that can be cheaply and easily treated. Data from the BRFSS (Behavioural Risk Factor Surveillance System, USA) suggest that 70% of the adult population do not follow the minimum AHA recommendations in terms of physical exercise: 30 minutes of mild to moderate physical activity at least 5 days/week or 20 minutes of intense activity at least 5 days/week (8).
A structured training program has proven to improve long-term adherence. In overweight and obese subjects, screening for coronary heart disease, symptoms and arrhythmias is recommended (exercise test) before a training program is established. In addition, this approach can help the physician establish baseline exercise capacity and maximal heart rate. In these patients, structured sessions of at least 35 minutes of exercise (5 pre-exercise, 20 minutes exercise, and 10 minutes post-exercise) 4-5 days a week are preferred.
2.2. Medical treatment
Contrary to other cardiovascular risk factors, there are no good drugs to treat obesity. Some medical treatments adjuvant to lifestyle modifications in patients with a BMI>30 kg/m2 have been suggested, especially for patients with obesity-related diseases. Rucker et al (9) recently published a meta-analysis assessing the efficacy and adverse effects of long-term therapies: orlistat, sibutramine, and rimonabant (Table 2). Orlistat, a gastrointestinal lipase inhibitor, reduced weight by 2.9% compared to placebo; almost all participants regained weight shortly. Sibutramine, a centrally acting monoamine reuptake inhibitor, reduced weight by 4.3% compared to placebo, and 10%-30% of the patients successfully maintained the weight loss. Patients receiving rimonabant, a CB1 endocannabinoid receptor antagonist, lost 4.7 kg more weight than those taking placebo, and maintained the weight loss. Apart from weight loss, these drugs also reduce abdominal circumference and systolic and diastolic blood pressure. Orlistat specifically reduced the incidence of diabetes mellitus, fasting glucose and glycosylated hemoglobin (HbA1c) concentrations in diabetics, total cholesterol, LDL-cholesterol and HDL- cholesterol (HDLc). Sibutramine and rimonabant reduced triglyceride concentrations and increased HDLc concentrations.
Current availability of these drugs is variable depending on the country (rimonabant has been withdrawn in most). Significant side effects and high rates of discontinuation have been observed. When medical therapy and lifestyle modification fail or the individuals are morbidly obese despite medical adjuvant therapy, other measures to induce weight loss are recommended, such as bariatric surgery.
2.3. Bariatric surgery
There are currently 2 main techniques for inducing significant weight losses in severely obese patients: vertical banded gastroplasty and Roux-en-Y gastric bypass.
Both are effective and safe techniques for achieving and maintaining weight loss in patients with morbid obesity or severe obesity with comorbidities such as coronary heart disease or respiratory function impairment (10).
More than half of patients who undergo bariatric surgery, especially those referred to gastric bypass, lose at least 50% of the excess weight (11). Some studies suggest that bariatric surgery can also significantly improve blood pressure, glycemia, lipid concentrations and quality of life (Figure 1). Nearly 70% of hypertensive patients achieve excellent or good control of blood pressure. About half of the diabetic patients who undergo bariatric surgery achieve normal HbA1c levels and can even stop using insulin or oral hypoglycemic agents. Patients undergoing bariatric surgery have a significantly reduced estimated cardiovascular risk, and some studies suggest that there may even be reductions in mortality following bariatric surgery (12). It has also been shown that left ventricular mass decreases and right ventricular function improves after weight loss following bariatric surgery (13); furthermore, bariatric surgery can slow down the deterioration in left ventricular diastolic function, as assessed by left atrial size (14). However, some studies that have assessed changes in left ventricular ejection fraction (the most currently used measure of cardiac function) have not demonstrated significant improvements following bariatric surgery. The causal association between weight loss and improvement in cardiac function remains to be established, to know whether is is due to improvement in diabetes, hypertension and/ or lipid control.
Table 1. Diagnostic Criteria for Obesity and Central Obesity
Underweight (Body mass index kg/m2 : under or equal to 18.5)
Normal weight (Body mass index kg/m2 :18.5-24.9)
Overweight (Body mass index kg/m2 : 25-29.9)
Obesity class I (Body mass index kg/m2 : 30-34.9)
Obesity class II (Body mass index kg/m2 : > or = 35)
Morbid obesity (Body mass index kg/m2 : > 40)
______________________________________________
Central obesity by abdominal circumference*
European and american men (Cutoff : > or = 102 cm)
European and american women (Cutoff : > or = 88 cm)
Asian men (Cutoff > or = 90 cm)
Asian women (Cutoff > or = 80 cm
________________________________________________
Central obesity by waist-to-hip ratio
Men >0.9
Women >0.85
According to the American Heart Association/National Heart, Lung and Blood Institute (Adult Treatment Panel III), these ranges are also recommended for white individuals; there is no evidence supporting the use of different values for Hispanic Americans, black Americans or American Indians.
*Recommended cutoffs for other groups: for the Japanese population, the Japanese Obesity Society suggests > or = 85 cm for men and > or = 90 cm for women; the Cooperative Task Force suggests > or = 85 cm for Chinese men and > or = 80 cm for Chinese women; the International Diabetes Association suggests > or = 94 cm for men and > or = 80 cm for women from Middle Eastern, Mediterranean and Sub-Saharan populations, and > or = 90 cm for men and > or = 80cm for ethnic Central and South American populations.
Table 2. Side effects of pharmacologic agents for the treatment of obesity
| Side effect | Orlistat | Sibutramin | Rimonabant |
| Fatty/oily stool | ++ |
||
| Fecal incontinence | ++ |
||
| Vitamin deficiency | + (Supplements required) | ||
| Raised blood pressure | + | ||
| Raised heart rate | + | ||
| Constipation | ++ | ||
| Insomnia | + |
||
| Dry mouth | + | ||
| Psychiatric disorders (anxiety, depression) | ++ |
Figure 1. Prevalence of risk factors before and after bariatric surgery / medical treatment (courtesy of Batsis JA) (10).
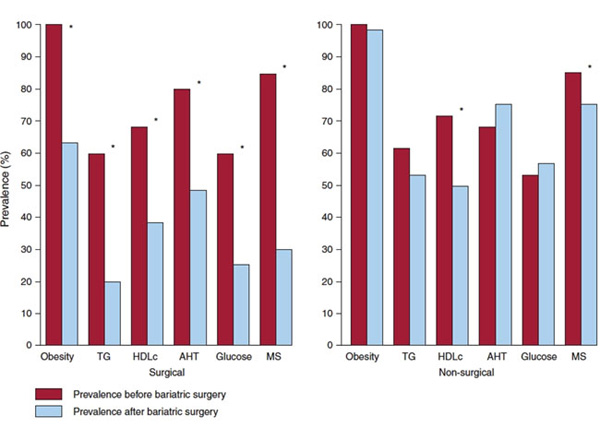
Change in the prevalence and in each of the 5 components of the metabolic syndrome as defined by the American Heart Association/National Heart, Lung and Blood Institute. Blue bars represent baseline prevalence, while red bars represent prevalence at follow-up. Significant changes (p less than 0.05) are represented by an asterisk. HDLc= high-density lipoprotein cholesterol; AHT= hypertension; MS= metabolic syndrome; TG= triglycerides.
Conclusion:
Obesity is a common cardiovascular risk factor to which physicians frequently ignore or treat dismissively. Excess weight is associated with many important cardiovascular diseases, not only coronary heart disease, but also abnormalities in heart rate and ventricular function. This association is due to multiple mechanisms, including hypertension, diabetes mellitus or dyslipidemia. The diagnosis of obesity should include measurements of total body fat content and its distribution. Although the management of obesity is difficult, a comprehensive management program can lead to favorable outcomes.
Physical activity and reduction in calorie intake should be encouraged in all patients. Moreover, bariatric surgery, when performed by experienced teams, has demonstrated excellent long-term results not only with regard to weight loss, but also in terms of risk factor modification and prognostic improvement. Office cardiologists should be aware of where, to whom, and when to indicate bariatric surgery for cardiovascular prevention.