
Background
Atrial fibrillation (AF) is the most common supraventricular tachyarrhythmia. It holds a five-fold risk of stroke and has important associated costs (1). Atrial fibrillation affects 1-2% of the general population and escalates to almost 15% in the eighth decade of life. Lone atrial fibrillation is AF in the absence of heart disease (while lone atrial fibrillation in the absence of any disease is termed "idiopathic"). Lone atrial fibrillation is more prevalent in younger males and is either paroxysmal, persistent or permanent. Its natural history still remains uncertain, so it is a diagnosis of exclusion, which should only be made after vigilant clinical assessment complete with ECG, Echocardiogram (echo) and TFTs (thyroid function tests) results. In LAF and idiopathic AF, atrial foci functioning as triggers are generally localised in the pulmonary veins (PVs). Various factors are involved in the onset, perpetuation and relapse of LAF. Autonomic disturbances hold the most profound links to lone atrial fibrillations, and trigger factors include hyperthyroidism, diabetes, genetic predisposition, obesity, sleep apnea, metabolic disturbances, alcoholism and mood disorder (2). Treatment is aimed at symptom relief and prevention of thromboembolic complications. A trial of medical therapy and/or percutaneous ablation may be offered prior to surgical intervention. Regular follow up with evaluation of cardiovascular risk factors is necessary in all lone atrial fibrillation patients.
Surgery
Surgical treatment modality is contingent on a number of individual factors: type and duration of AF, LA size and degree of atrial remodeling. These factors will help to determine the suitability and success of the intervention. A summary of the main indications for surgical intervention in LAF are as follows.
- Permanent or persistent AF of long duration with large LA size (>5cm).
- Intolerant arrhythmias refractory to medical therapy and/or percutaneous ablation. Permanent AF is usually stable however paroxysmal AF is frequently symptomatic and necessitates surgical intervention.
- AF patients with contraindication to long-term anticoagulation (e.g. intracranial hemorrhage). Patients taking Warfarin have twice the rate of intracerebral hemorrhage and associated mortality relative to the intensity of anticoagulation. AF patients on anticoagulants have an incidence of 2.3% per annum for major hemorrhage, and 0.9% per annum for intracranial bleed (3).
- Tachycardia-induced cardiomyopathy (TIC) in patients with AF. TIC is defined as atrioventricular dysfunction caused directly by tachycardia in a structurally normal heart (4). Surgical restoration to sinus rhythm (SR) can revert the TIC. TIC should highly be suspected in patients with uncontrolled AF presenting with heart failure.
- Recurring cerebrovascular events in patients with permanent AF despite adequate anticoagulation: Warfarin significantly lowers the peril of thromboembolic stroke to 60% in patients with AF but does not exclude this dreaded complication. A retrospective study at Barnes-Jewish hospital discovered that 20% of patients undergoing the Cox-Maze III procedure had at least one incidence of substantial temporary or permanent neurologic deficit preceding the procedure due to cerebral thromboembolism (5).
- Patients with left atrial thrombus. Catheter based ablation is contraindicated in LA thrombus and surgical removal of the thrombus, exclusion of LA appendage and surgical ablation is recommended.
- Young patients with intractable LAF who prefer a surgical approach and wish to avoid chronic medical therapy.
- Significant side effects, intolerance and contraindications to antiarrhythmic drugs (AADs). These drugs are notorious for increasing the risk for drug-induced life-threatening arrhythmias e.g. torsade de pointes, and certain AADs are also associated with serious side effects such as thyroid and pulmonary toxicity. This results in a significant compromise in quality of life and functional status. Surgery may play a vital role if catheter intervention is unsuccessful.
Techniques and results
Altogether, surgery is the mainstay for LAF refractory to medical therapy and/or failed catheter based intervention(s). Although standalone surgical intervention has not yet become a standard practice, it is progressively increasing in numbers. Indeed, surgery:
- Takes supremacy in easily attaining complete isolation with transmural lesions over catheter intervention (1).
- Allows left atrial appendage (LAA) exclusion/excision, which is regarded, as one of main advantages of surgery (6, 9).
- Is easier to perform. Current ablation technologies using alternative energy sources that replicate the surgical maze allow quicker, more effective and lesser invasive procedures on a beating heart (1).
- Avoids exposure to fluoroscopic radiation, and the added risk of thromboembolism, endocardial trauma related to catheter interventions.
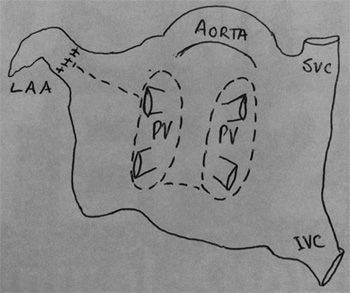
The original cut and sew Maze procedure is very difficult and time consuming. In order to make the procedure simpler, easier to perform and with advent of technology, investigators developed modifications. Kress et al have endorsed one such left atrial lesion set for the treatment of atrial fibrillation (7) as shown below.
Fig. 1. LA Maze procedure: The broken lines represent ablative lesions made by an alternative energy source
The exceptional results of Cox-Maze procedure mark it the gold standard, amid 75-95% success rate and freedom from AF up to 15 years. Mokadam et al in their multicenter trial of the Cox-Maze IV procedure revealed comparable outcomes as 96% of patients were free of AF at 6 months alongside zero operative mortality (8).
Niv Ad et al demonstrated a near 15% improvement in left ventricular (LV) function within 6 weeks following surgical restoration to SR in patients with poor pre operative LV function (i.e. ejection fraction (EF) <40%). Physical functioning health related quality of life scores improved with no stroke at 12 months with 19% of subjects having undergone stand-alone Cox-Maze for LAF (9).
Video-assisted interventions
Video-assisted interventions have been shown to result in a higher rate of conversion to SR and lower operative risks (10). Numerous studies have confirmed the safety and efficacy of bilateral, video-assisted, thoracoscopic pulmonary vein (PV) isolation with excision of the LAA (11). Sagbas et al evaluated the feasibility of a new off-pump technique of bilateral thoracoscopic pulmonary vein (PV) isolation for LAF, finding it safe and 100% effective for paroxysmal LAF (12).
Post-operative follow-up
Post operative antiarrhythmic and anticoagulants are continued for at least 3 months and up to 12 months./ They are subsequently withdrawn on maintenance of SR based on clinical, ECG, and echocardiographic assessment at 3, 6 and 12-month follow-ups (1). The surgical approach may, in some cases be ineffective as certain patients with post-operative residual or recurrent LAF may need antiarrythmics for rate control or maintenance of sinus rhythm beyond the initial post operative period. In the absence of prospective, randomised controlled trials in patients with LAF, definitive guidelines are still being developed.